58章 抗核抗体 Anti-nuclear Antibodies

キーポイント
リウマチ性疾患の中で、抗核抗体(ANA)はSLE、全身性硬化症、炎症性筋炎、原発性シェーグレン症候群に特徴的である。薬物誘発性ループスなど、いくつかの症候群の診断にはANAの存在が必要である。蛍光ANA検査はこのような疾患が疑われる場合のスクリーニング検査として適切である。
多くのANA特異性は一般的に疾患特異的、あるいは症状特異的と考えられているが、例外はよく知られており、多くの自己抗体が健常者では低い頻度で存在する。
理想的には、個々のANA特異性の検査は、抗体と疾患との関連(例えば、ループス腎炎に対する抗DNA)に相関する臨床症状との関連においてのみ実施されるべきであるが、多くの臨床検査室でANAパネルが利用可能になり、実施されるようになった結果、臨床的意義が不確かな状況でも特異的なANA検査が実施されることがしばしばある。その結果、ANAおよびANA特異性検査は、診断の確定や反論には不十分である。
はじめに
抗核抗体(ANA)には、複数の細胞内抗原に対する多様な自己抗体が含まれ、分類上はDNAや小核リボヌクレオタンパク 質(snRNP)などの核特異性からなるが、後に有糸分裂紡錘体、 サイトゾル、細胞質小器官、細胞膜など、他の様々な細胞構成成分にも拡大した。抗核抗体関連疾患は、蛍光ANA(FANA)検査でしばしばスクリーニングされる、しかし、ANAは健常人だけでなく、様々な感染性疾患、炎症性疾患、腫瘍性疾患でも発現するため、適切な臨床利用のためには、その複雑さと検査法の限界に関する知識が必要である。一部の臨床検査室では、標的自己抗原特異性の予測におけるFANAパターンの役割は、広く利用されている自己抗原特異的ELISAに取って代わられている。
多くの疾患が抗ssDNA活性を示すが、SLEだけが特徴的に高力価の抗dsDNA活性を有している
Comment: “most clinical literature remains linked to classic anti-dsDNA antibodies; many diseases exhibit anti-ssDNA activity, but only SLE sera characteristically possess high-titer anti-dsDNA”
抗DNA抗体の中には、他の自己抗原と交差反応するものもあり、神経細胞のN-メチル-D-アスパラギン酸(NMDA)受容体や中枢神経系疾患のリボソームP抗原など、他の末端臓器症状との相関を説明することができる。その結果、抗DNA活性の存在は常に腎疾患を考慮すべきであるが、抗DNA活性の存在が常にループス腎炎を示すとは限らず、その逆もまた然りである。実際、臨床的に一貫性がない場合、抗dsDNA抗体の予後予測能は低い(Scand J Rheumatol. 2013;42(4):311-6.)
Comment: “Some anti-DNA antibodies may cross-react with other autoantigens, explaining correlation with other end-organ manifestations, such as the neuronal N-methyl-D-aspartate (NMDA) receptor or ribosomal P antigens for CNS disease.33,34 Such findings suggest that the immunologically relevant antigen for anti-DNA antibodies may not in fact be DNA. Indeed, in inconsistent clinical settings, anti-dsDNA antibodies have low prognostic value.”
・ADNAが陽性でも臨床症状がない人では、5年後に1/36しかSLEを発症しませんでした。(Scand J Rheumatol. 2013;42(4):311-6.)
抗ヒストン(ヌクレオソーム)抗体は、転写不活性クロマチンの下部構造を形成するDNA-蛋白複合体であるヌクレオソームの蛋白成分を標的とする。抗ヒストン抗体はSLEによくみられ、抗dsDNA抗体と結合し、抗ssDNA抗体と結合する薬物誘発性ループスに特徴的である。
Comment: “Anti-histone (Nucleosome). Anti-histone antibodies target the protein components of nucleosomes, the DNA-protein complexes that form the substructure of transcriptionally inactive chromatin. They are common in SLE, associate with anti-dsDNA, and are particularly characteristic of and sensitive for drug-induced lupus, where they associate with anti-ssDNA.29 However, they are commonly seen in other rheumatic diseases, including myositis and SSc, as well as chronic infections, such as Epstein-Barr virus, and as a result clinical correlations for anti-histone antibodies have not been consistent.“
Ro52単独陽性はpSSと相関するが、Ro60はRo52に関わらず、SLEを含む他のCTDと相関する。
Comment: “Ro52 without Ro60 specificities correlates with pSS, whereas Ro60, perhaps specifically a Ro60 apoptope, with or without Ro52 specificities, correlates with other CTDs, including SLE. (Autoimmun Rev.2009 Jun;8(7):632-7.)”
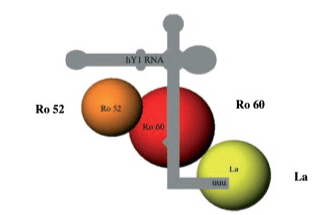
Ro(SS-A)はRo52かRo60
Ro(SS-A)とLa(SS-B)
抗Ro抗体はpSS患者の約40%から95%に認められ、抗La抗体やリウマチ因子との血清学的関連など、多くの腺外症状と関連している。同様に、抗La抗体はpSS患者の87%に認められる
https://www.sciencedirect.com/science/article/abs/pii/B9780123749949100154
n=399
・43.1% が Ro52 + Ro60-
・32.6% が Ro52 + Ro60+
・24.3% が Ro52-Ro60+:SLEが最も頻繁に診断された (48.5%)、一方SjSは少なかった(13.4%)
SLE(n=122)の17%はRo52 + Ro60-、44%はRo52+ Ro60+、38%はRo52- Ro60+
SjS(n=76)の15%はRo52 + Ro60-、67%はRo52+ Ro60+、17%はRo52- Ro60+
炎症性筋疾患(n=18)の72%はRo52 + Ro60-、5%はRo52+ Ro60+、22%はRo52- Ro60+
Front Immunol. 2019 Mar 12;10:444.
・抗核抗体のパターンの違い
Ro52: nuclear fine speckled
Ro60: myriad discrete nuclear speckles (AC-4a)
https://www.anapatterns.org/view_pattern.php?pattern=4
J Immunol Methods. 2013 Apr 30;390(1-2):35-40.
RNAP III抗体は、皮膚スコアの上昇、腱摩擦、腎クリーゼを含むびまん性皮膚SScを予測する可能性があり、特に肺がんリスクの上昇と関連している(Arthritis Rheumatol.2014 Feb;66(2):407-17.)。
Comment: “ RNAP III antibodies in particular may predict diffuse cutaneous SSc, including higher skin score, tendon friction rubs, and renal crisis, and are associated with an increased risk of cancer, particularly of the lung.”
特に肺がんなんですね。
抗U1 snRNP抗体の存在は、分類や診断に一貫して必要とされており、関連するANA抗体価は通常1:1000を超え、しばしば1:10,000である(Rheum Dis Clin North Am. 2005 Aug;31(3):437-50)
Comment: “ the presence of anti–U1 snRNP antibodies has been consistently required for classification and/or diagnosis, with associated ANA titers typically exceeding 1:1000 and often 1:10,000.“
力価が高い。
レイノー症状陽性の場合、SLE、RA、SScを含む全身性リウマチ性疾患を発症する可能性が19%から30%高くなるが、陰性の場合、その可能性は約7%に低下し、患者の安心に役立つことが多い(Arthritis Rheum. 2008 Dec;58(12):3902-12.)
Comment: “In RP, a positive result increases the likelihood, from 19% to 30%, of the development of a systemic rheumatic disease, including SLE, RA, and SSc, whereas a negative result decreases the likelihood to approximately 7%, which is often helpful for patient reassurance.”
FANA陽性の場合は通常、特異抗体検査による経過観察が必要となる。なぜなら、ANAが臨床的疾患より何年も先行しているためである(N Engl J Med. 2003 Oct 16;349(16):1526-33.)。CTDの他の臨床的徴候がない場合のANAの陽性適中率は、低い。
Comment: “A negative or low-titer FANA in the setting of a low clinical suspicion of rheumatic disease usually indicates the absence of significant ANAs and argues against the diagnosis of one of the ANA diseases; however, if the clinical picture strongly suggests CTD, further investigation may involve specific assays for antigens that are often FANA negative, such as Ro/SS-A, Jo-1, or phospholipids. but only in the setting of strong clinical suspicion, because the positive predictive value of an ANA in the absence of other clinical signs of CTD is low, in part because ANAs may precede clinical disease by many years, and in part because of the relatively high incidence of ANA in healthy people. Thus, if SLE features are present, further work may focus on anti-DNA, anti- Sm, anti–RNP/U1 snRNP, and anti-Ro antibodies. “
・健常人でもANA 1:40 で 31.7%、1:80 で 13.3%、1:160 で 5.0%、1:320 で 3.3% が陽性でした。
(Arthritis Rheum. IF: NANA1997 Sep;40(9):1601-11.)

N Engl J Med. 2003 Oct 16;349(16):1526-33.
SLE発症の5年も前からdsDNA抗体は陽性になっている。
この業界では大変有名な論文ですね。
この記事が気に入ったらサポートをしてみませんか?