50章 腰の痛み Low Back Pain

キーポイント
腰痛(LBP)は80%もの人が罹患しており、腰椎の退行性変化が最も一般的な原因である。
これらの患者の90%以上は8週間以内にほとんど痛みがなくなるが、再発することも多い。
初期評価では、神経病変、骨折、全身性疾患(感染症、悪性腫瘍、脊椎関節炎)の可能性がある少数の患者を特定することに重点を置くべきである。
画像異常は、加齢に伴う退行性変化の結果であることが多いが、無症状の人にみられることが多いため、慎重に解釈すべきである。
痛みの発生源を特定する正確な病理解剖学的診断は、患者の85%までは不可能である。
持続性のLBPは、鎮痛、体幹強化、ストレッチング、有酸素運動によるコンディショニング、過剰体重の減少、患者教育など、個々に合わせたプログラムで治療すべきである。
保存的治療がうまくいかない場合は、認知行動療法に重点を置いた集学的な集中リハビリテーションを強く考慮すべきである。
椎間板ヘルニアに続発する神経根症がない患者に対する硬膜外コルチコステロイド注射の有効性を示す証拠はない。
腰部手術の主な適応は、重篤または進行性の神経学的障害の存在である。
神経学的欠損がない場合、背部手術、特に変性変化に対する脊椎固定術は、保存的治療よりも有効ではない。
疫学
腰痛(LBP)は、臨床医学において最もよく遭遇する疾患のひとつである。腰痛は、胸郭下部と臀部の間の領域に影響を及ぼす。
LBPは人生の最初の10年間はまれであるが、10代で急激に増加する。有病率は、60~69歳まで年齢とともに増加し、その後徐々に減少する。
2015年の世界における5億4,000万人が常時罹患していることになる。LBPは現在、世界的に障害の原因の第1位であり、慢性疼痛症候群の中で最も多く、45歳未満の患者における活動制限の主な原因となっている。米国では、LBPによる労働損失日数は、他のどの職業性疾患よりも多い。
急性腰痛症は、ほとんどの患者で4週間以内に改善し、8週間後には90%以上が改善する。残りの7~10%は、慢性的に持続する。
解剖
腰椎は5つの椎骨からなる。各椎骨は、前方に椎体、後方に脊柱管を囲む神経弓からなる。
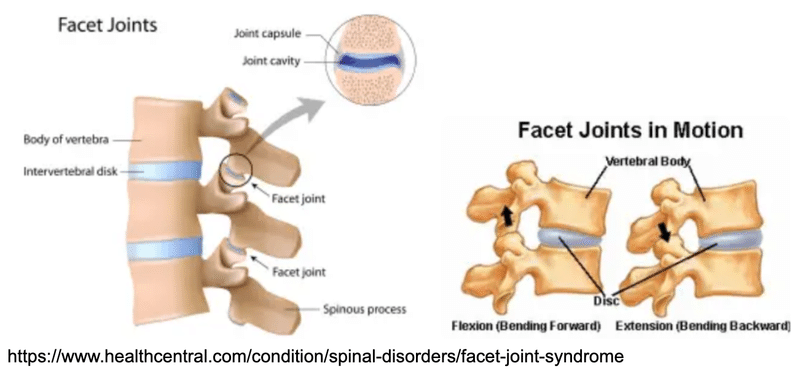
腰椎には、前方に配置された椎間板関節(椎間板と隣接する椎骨によって形成される)に加えて、後側方の椎間関節(facet joint)がある。これらは、隣接する椎骨の上関節突起と下関節突起が結合して形成される。
椎間関節痛は、診断的治療としてその部位にブロック注射による痛みの改善をみることができる。
腰椎ではfacet jointsの痛みが多いようです。
Pearl: 炎症性腰痛の有病率(3%~6%)と脊椎関節炎の有病率(0.4%~1.3%)の差は、炎症性腰痛がしばしば治るという事実によって説明できるかもしれない(Arthritis Rheumatol 70(7):1049–1055, 2018.)
Comment: “The fact that inflammatory back pain often resolves may explain the difference between the prevalence of inflammatory back pain (3% to 6%) and the prevalence of spondyloarthritis (0.4% to 1.3%).”
炎症性背部痛の既往を軸性炎症のマーカーとして過大視できないということですね。
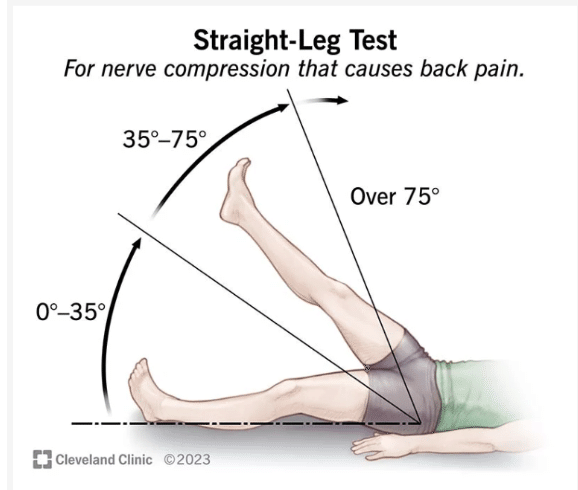
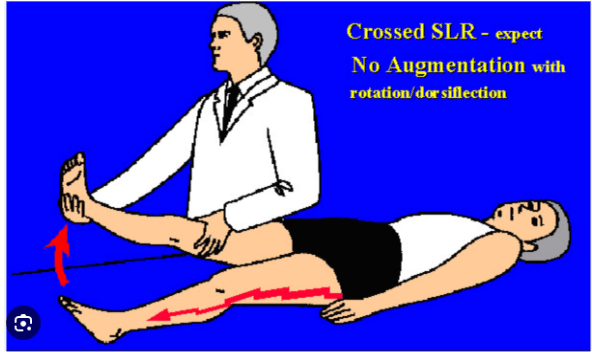
Pearl: L4-5またはL5-S1レベル(臨床的に意味のある椎間板ヘルニアの95%の部位)の椎間板ヘルニアに対して、straight leg–raising testの感度(91%)は高いが特異度(26%)は低い。一方、脊柱管狭窄症患者では、straight leg–raising testは通常陰性であるが、交差直立挙上テスト(反対側の脚を挙上すると坐骨神経痛が再現される)は、非常に特異的である (Cochrane Database Syst Rev. 2010 Feb 17;(2):CD007431.)。
Comment: “Dorsiflexion of the ankle further stretches the sciatic nerve and increases the sensitivity of the test. Pain experienced in the posterior thigh or knee during straight leg raising is generally from hamstring tightness and does not represent a positive test. The straight leg–raising test is sensitive (91%) but not specific (26%) for clinically significant disk herniation at the L4-5 or L5-S1 level (the sites of 95% of clinically meaningful disk herniations). False-negative tests are more frequently seen with herniation above the L4-5 level. The straight leg–raising test is usually negative in patients with spinal stenosis. The crossed straight leg–raising test (with radicular pain reproduced when the opposite leg is raised) is highly specific but insensitive for a clinically significant disk herniation.”
Pearl: つま先歩き(主にS1)と踵歩き(主にL5)ができない場合は筋力低下を示す。
Comment: “The inability to toe walk (mostly S1) and heel walk (mostly L5) indicates muscle weakness”
Pearl: 重大な腰痛症状が6~8週間以上持続しない限り、画像診断は必要ない。患者の90%以上が8週までにほぼ回復しているため、不必要な早期検査を避けることができる
Comment: “Otherwise, imaging is not required unless significant symptoms persist beyond 6 to 8 weeks. “.
・発熱、体重減少などのレッドフラッグがなければまずは様子みましょう、ということですね。どうしても原因を探りたくなっちゃいますが。
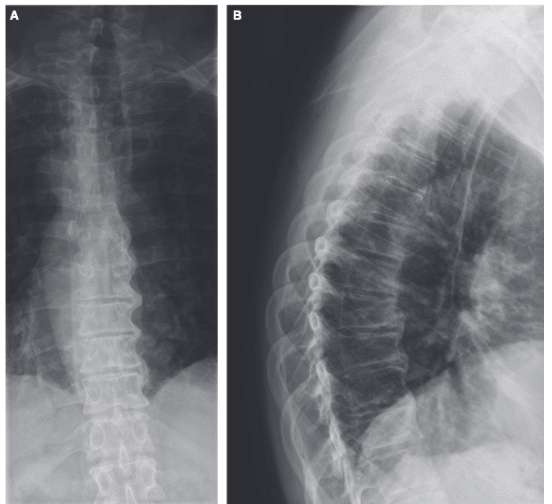
Pearl: 通常、腰の評価には立位Xpでの前方視と側方視で十分である。斜位視は、放射線被曝を増加させるだけで、新たな診断情報をほとんど追加しない。腰椎の2方向X線写真による女性の性腺被曝は、1年以上毎日撮影した胸部X線写真による被曝と同等である(Ann Intern Med. 2007 Oct 2;147(7):478-91.)
Comment: “Standing anteroposterior and lateral views are usually adequate. Oblique views substantially increase radiation exposure and add little new diagnostic information. Gonadal radiation in a woman from a two-view radiograph of the lumbar spine is equivalent to radiation exposure from a chest radiograph taken daily for more than 1 year.”
斜位は腰椎滑り症を診断する際の、関節間部の欠損(pars interarticularis defect)を確認するために撮影される条件ですが、最近はCTやMRIに取って代わられているようです。
Pearl: 仙腸関節のMRIにおける骨髄浮腫の存在は、しばしば軸性脊椎関節炎の特徴であると考えられている。しかし、(仙腸関節炎の定義を満たす)低グレードの骨髄浮腫は、健常人(25.5%)、慢性機械的LBP患者(10.6%)、長距離ランナー(16.7%)、産後腰痛の女性(57.1%)にみられることがある。しかし、深部骨髄浮腫と関節びらんの存在は、軸性脊椎関節炎の特異性を有意に高める(Arthritis Rheumatol 70(7):1042–1048, 2018)
Comment: “The presence of bone marrow edema on MRI of the sacroiliac joints is often considered a hallmark of axial spondyloarthritis. However, low-grade bone marrow edema (that fulfills the exist- ing definitions of sacroiliitis) may be seen in healthy individuals (25.5%), patients with chronic mechanical LBP (10.6%), long distance runners (16.7%), and women with postpartum back pain (57.1%). The presence of deep bone marrow edema and joint erosions are, however, significantly more specific for axial spondyloarthritis.“
Pearl: DISHでは、椎体の前方および右外側に、骨化した靭帯が靭帯内骨棘といっしょに流れる蝋のように見える。逆位患者では左外側に石灰化がみられるが、このことから下行大動脈が石灰化の発生部位に関与していると推測される。
Comment: “The ossification, together with bridging enthesophytes in the spine, give the appearance of flowing wax on the anterior and right lateral aspects of the spine. Involvement of the left lateral aspect in patients with situs inversus has led to speculation that the descending aorta plays a role in the location of the calcification.”
膝蓋骨、肘頭突起、踵骨などの付着部位の腱や靭帯、骨盤X線写真における寛骨臼外側や仙腸関節下部のような関節周囲の骨棘も認められることがある。
Pearl: 椎体炎においては、ほとんどの患者が鎮痛薬を使用していることもあり、発熱は患者の約半数にしかみられない。白血球増加は患者の約3分の2にしかみられない。しかし、ほとんどすべての患者にESR、CRPの増加がみられ、後者は治療に対する臨床的反応と最もよく相関する。
Comment: “Fever is present in only approximately half of the patients, in part because most patients are using analgesic medications. Leukocytosis is seen in only approximately two-thirds of the patients. However, almost all the patients have increases in the erythrocyte sedimentation rate and C-reactive protein, with the latter best correlating with clinical response to therapy.”
・血液培養は50~70%の患者で陽性である。
・化膿性骨髄炎の典型的な所見は、2つの椎体とその間にある椎間板の浸潤である。神経障害のある患者では、硬膜外膿瘍を除外するために早期にMRIを行うべきである。

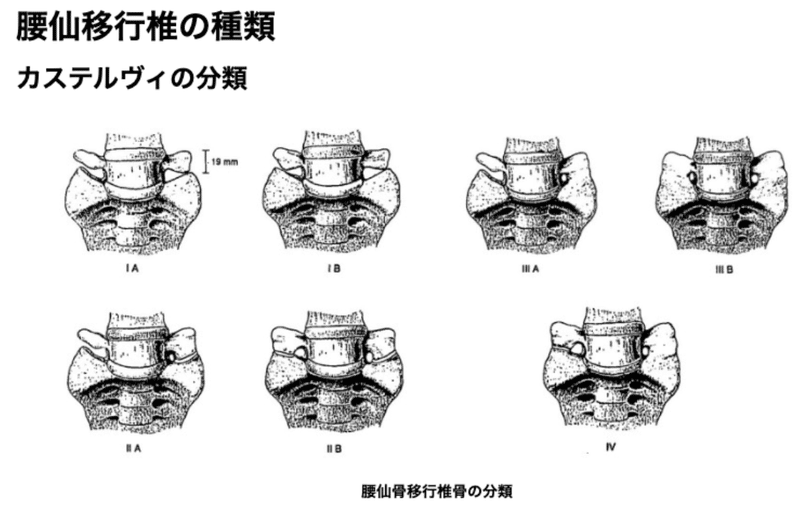
Pearl: 腰仙移行椎には、最下位腰椎の仙骨化(L5が仙骨に同化し、4つの腰椎と拡大した仙骨分節になる)と最上位仙骨分節の腰椎化(S1が腰椎に同化し、6つの腰椎と短縮した仙骨分節になる)がある。これらの一般的な変異は、一般人口の15%~ 35%にみられる。
Comment: “Lumbosacral transitional vertebrae include sacralization of the lowest lumbar vertebral body (assimilation of L5 to the sacrum resulting in four lumbar vertebrae and an enlarged sacral segment) and lumbarization of the uppermost sacral segment (assimilation of S1 to lumbar spine resulting in six lumbar vertebrae and a shortened sacral segment).”
Pearl: 硬膜外脂肪腫症は、肥満患者にみられることがあるが、副腎皮質ステロイドの長期使用のまれな副作用としてみられることが多い。硬膜外脂肪組織の増加により脊柱管が狭窄する。
Comment: “Epidural lipomatosis may be seen in obese patients, but it is more commonly seen as a rare side effect of long-term use of corticosteroids.”
腰痛で発症
脂肪腫症は、コルチコステロイド治療の平均 1.3 (+/- 1.5) 年 (SD) (中央値、0.8 年、範囲、3 週間~6.5 年) 後に発現した。脂肪腫症の発症時のコルチコステロイドの投与量は広範囲にわたり、プレドニゾン 5 ~ 80 mg/日。腰痛が最も一般的な症状。画像検査により、脂肪腫症はほとんどの場合胸椎に関与しており、一部の患者では腰仙骨領域にまで広がる。
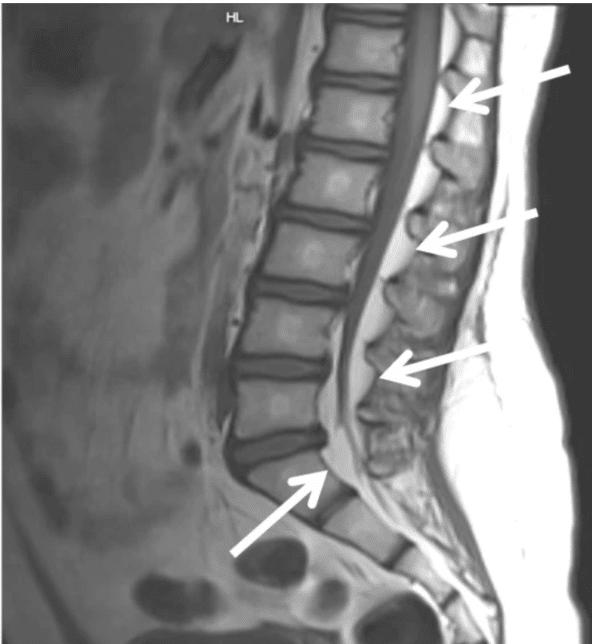
リスク因子は長期間のステロイド投与(期間は不明)、肥満です。
Global Spine J. 2019 Sep; 9(6): 658–665.
Pearl: バックマウスは、腰仙部にできる可動性の皮下線維脂肪性結節である。結節は圧痛を伴うことがある。LBPと "back mouse "を合併した患者の症例報告があるが、LBPとの関連はまだ証明されていない。
Comment: “A “back mouse” is a mobile subcutaneous fibro-fatty nodule in the lumbosacral area. The nodule may be tender. Although there are case reports of patients with LBP and “back mice,”82 the association with LBP remains unproven.”
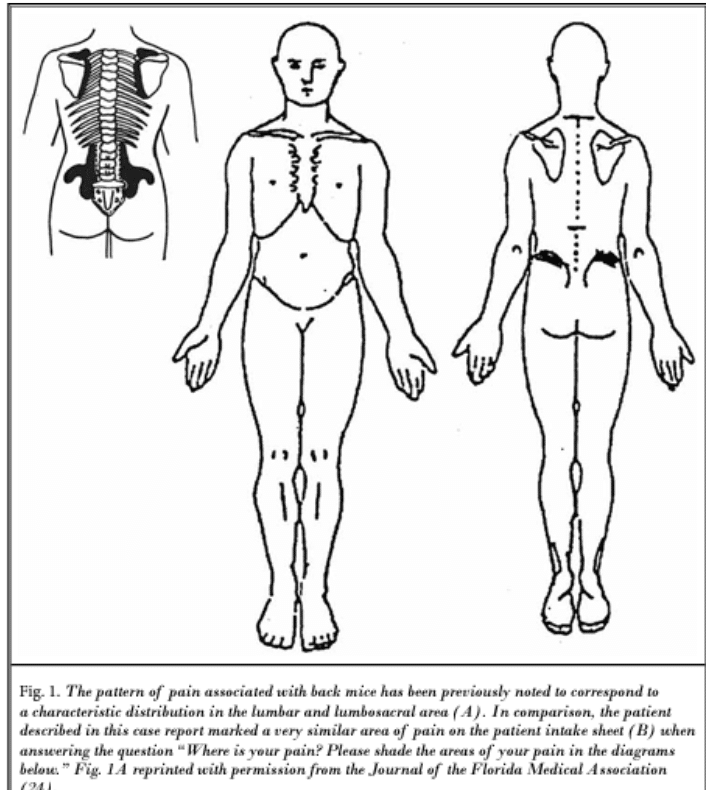
仙腸関節、後上腸骨、腰部傍脊柱の特徴的な部位にみられる固いゴム状の可動性結節は、筋膜層を介してヘルニア化した脂肪組織である可能性がある。
Episacral lipomaなどと呼ばれることもある。
Pain Physician 2016; 19:181-188
この記事が気に入ったらサポートをしてみませんか?