【大腸】鋸歯状病変レビュー2011:鋸歯状病変診断の本質に迫る

Update on the serrated pathway to colorectal carcinoma
Dale C. Snover. Human Pathology (2011) 42, 1–10
Summary
Adenocarcinoma of the large intestine can no longer be considered one disease but rather a family of diseases with different precursor lesions, different molecular pathways, and different end-stage carcinomas with varying prognoses. Approximately 60% of colorectal carcinomas arise from conventional adenomas via the suppressor pathway leading to microsatellite stable carcinomas. These carcinomas represent the pathway that has been the target of screening and prevention programs to date. However, approximately 35% of carcinomas arise along the serrated pathway developing from the precursor lesion known as the sessile serrated adenoma (also referred to as the sessile serrated polyp). Sessile serrated adenomas/polyps lead to carcinomas with extensive CpG island promoter methylation (CpG island methylated phenotype positive carcinomas), which can be either microsatellite instable high or microsatellite stable. The remaining 5% of carcinomas arise from conventional adenomas in patients with germ line mutations of mismatch repair genes (Lynch syndrome), leading to CpG island methylated phenotype negative microsatellite instable carcinomas. Carcinomas arising from sessile serrated adenomas/polyps are not prevented by removing conventional adenomas and hence may be missed in routine screening programs. In addition, a subset of these lesions may potentially progress rapidly to carcinoma; hence, it is likely that these lesions will require a different screening strategy from that used for conventional adenomas. This article reviews the various pathways to colorectal carcinoma with emphasis on the serrated pathway and evaluates the implications of this pathway for colorectal carcinomas screening programs.
アブストラクトおよび本文の主旨は、鋸歯状病変を分子生物学的観点から再分類しようということである。しかし、これが 2011 年の論文で、2019 年に最新の消化器 WHO 分類が出ていて、ここで挙げられている terminology は新 WHO 分類には採用されていない(疾患分類のコンセプトは同じである)。むしろ、この論文は鋸歯状病変を診断する、つまり目の前の標本に当てはめて分類するに当たって、最も本質的な内容が記載されている点で非常に有益である。各鋸歯状病変の分子生物学的背景に伴う特徴、その結果としての形態的特徴を以下に【SANOTIC SUMMARY】として挙げる。
【SANOTIC SUMMARY】
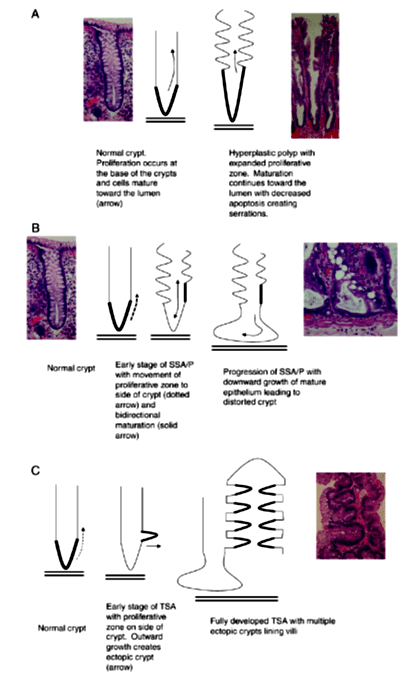
各鋸歯状病変の本質は、
(1)HP:陰窩底部の増殖帯の延長
👉腺管内腔に細胞が重責して鋸歯状になる
(2)SSA/P(SSL):陰窩の増殖帯の延長+左右不均等
👉増殖帯の位置異常による陰窩の不規則変形
(3)TSA:陰窩底部と粘膜筋板の接着性 anchoring の消失
👉陰窩と垂直方向に微小陰窩が飛び出す
👉多数の微小陰窩による鋸歯状の形態
👉粘膜筋板から離れて陰窩が増殖する
👉その結果全体がウネウネ絨毛状となる
※ TSA における微小陰窩の飛び出しを「陰窩の芽出(crypt budding)」あるいは「異所性陰窩形成(ectopic crypt formation/foci:ECF)」と呼ぶ。
である。他にも細かな診断基準があるが、それらは枝葉であり、ここに挙げた内容が診断に際して最も重要な本質である。
過去のオススメ論文はこちら👇
医学関連サイトマップ【SANOTIC ARCHIVES】👇
【病理医さのーと】についてはこちら👇
サポートいただいた分は、サポートに使います。サポートの輪ができていくのに少しでも貢献できればと思います😊